THE HORSEMEN OF THE APOCALYPSE,
A MICROSCOPIC VIEW. PART I
MANUEL del CERRO, USA,
INTRODUCTION
The Apocalypse attributed to John of Patmos (John the Divine), also called the Book of Revelation, is the last canonical book of the New Testament in the Christian Bible [1]. Prominent in the narrative are the so-called Horsemen of the Apocalypse, mounted knights that run the Earth disseminating sorrow and death (Figure 1).
Theology is not one of my fields of exploration, but I think I may have found the microscopic equivalent of Horsemen of the Apocalypse and would like to share that finding with fellow microscopists.
Figure 1. The Horsemen of the Apocalypse in an early Renaissance version. (Woodcut by Albrecht Dürer, 1471–1528)
MICROSCOPIC VIEW
I have recently acquired (2008) a set of slides that show tissues infected with the microbes of anthrax, leprosy, syphilis, tuberculosis, and an opportunistic fungal infection in an AIDS patient. These infectious agents are the microscopic equivalents of the Horsemen that spread death and sorrow. Since the subject of infectious disease is of general interest, I will comment on the slide set, on each of the individual slides, and briefly, on the corresponding disease.
THE SLIDE SET
These five slides (Figure 2) were sold as a set on eBay in August 2008. They are sections of tissues heavily infected with the agents of anthrax, leprosy, syphilis, tuberculosis, and with Pneumocystis carinii. As for technical information, I only have that provided on the label of each slide, complemented by the examination of the slides under the microscope. The slides are signed with the initials A. J. D. These initials correspond to the name of Anthony J. DiDonato. Mr. DiDonato, from Philadelphia, is widely known as a most prolific photomicrographer. These slides attest to his proficiency as histotechnologist and slide mounter as well. [Disclaimer: I never met Mr. DiDonato and have no monetary interest in his work].
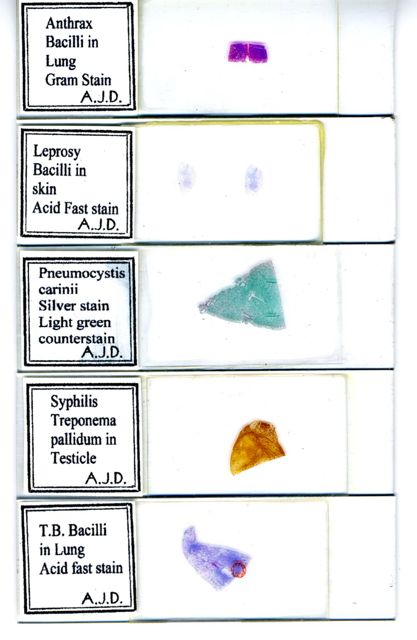
Figure 2. Scanned image of the set of slides.
SLIDE 1. ANTHRAX INFECTION OF THE LUNG.
Anthrax is a disease that has been recently in the news for some very unfortunate reasons. It was known as a disease of livestock since the Classical Antiquity (Virgil, Georgics, 29 BC), and it was not much later that human infection was also recognized, making of this a zoonotic disease (one shared by animals and humans). Its causative agent is Bacillus anthracis, a gram-positive, spore-forming, facultative anaerobic bacteria (one able to live with little or no oxygen if needed). There are cutaneous, intestinal, pulmonary, and meningeal forms of the disease [2]. This slide shows the pulmonary form. Typically, pulmonary anthrax starts with chest pain, low fever, and dry cough. As the disease advances there are breathing difficulties, high fever, and low blood-oxygen levels, as evident by bluish coloration of the skin. In severe cases the patient experiences profound respiratory distress. Comparison between the lung seen in Figure 3, and that of a normal lung (Figure 4) explains why.
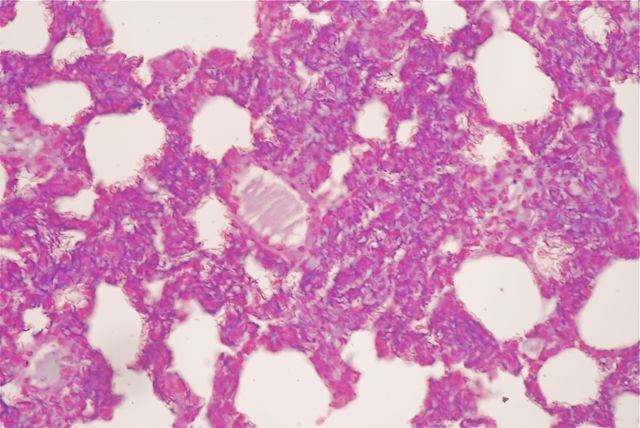
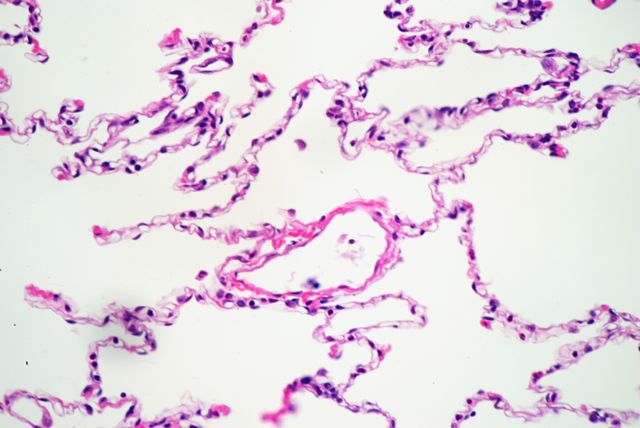
Figures 3 and 4. Microscopic views of the anthrax-infected lung (top) and of a normal lung (bottom). Both pictures were taken at the same magnification and under the same conditions. The empty areas in both are the respiratory alveoli or air sacs; these receive inhaled air and allow oxygenation of the circulating blood. The density of those empty sacs is considerably lower in the anthrax-infected lung; hence, the respiratory distress experienced by the patient. Occlusion of blood vessels by heavily infected blood clots compounds the situation (Figures 5 A & B). Field width for pictures 3 & 4 is 420 µm.
[A description of the photographic technique used to obtain these and all other photomicrographs is given in the Appendix]
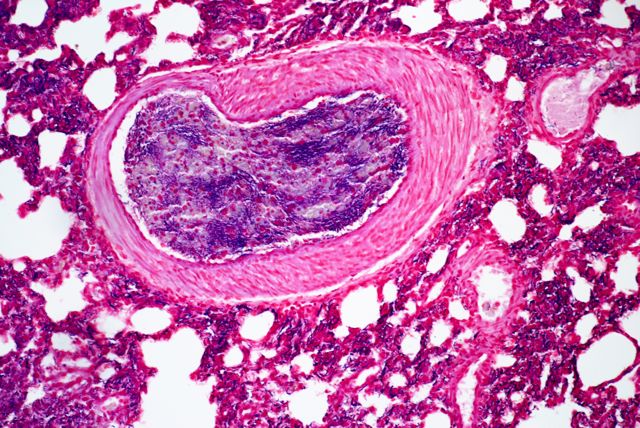
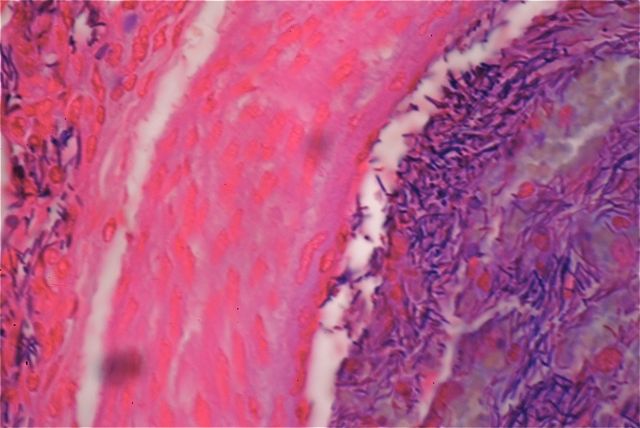
Figure 5 A & B. A blood vessel (V) is seen in a panoramic view in A, and at higher magnification in B. A) The lumen of the vessel is occluded by a blood clot. The field width is 420 µm. B) The blood clot and the lung tissue around it are infiltrated by an incredible number of deeply stained anthrax bacilli (thin, short, darkly stained rods); the fact that the section is relatively thick emphasizes this fact. The stain is superb. The field width is 170 µm.
SLIDE 2. LEPROSY LESION OF THE SKIN
Leprosy has been known for millennia. For almost as long, leprosy has been feared and misunderstood, thought to be a hereditary disease, a curse, or the expression of divine punishment. The patients were shunned from contact with their communities; they often were segregated into colonies, sometimes under dismal conditions. It is sad to recognize that all that unnecessary extra suffering was imposed on the patients for no valid medical reason - leprosy is minimally contagious!
Clinically, the disease is a chronic, progressive (if untreated) inflammatory process that affects preferentially the upper respiratory mucosa, the skin (Figure 6), and the nerves. The nerve lesions, leading to loss of sensation, are indirectly responsible for the progressive aggravation of unfelt wounds that may lead to ulcerations or even to loss of fingers. Leprosy does not express itself with the same intensity or lesion distribution in all patients; thus a number of classifications were devised trying to distinguish between the different forms. Recently, the World Health Organization has replaced a widely used classification that recognized six forms with a new one that recognizes only two: the pauci-bacillary and the multi-bacillary. This is based on the presence of few or many bacilli in the affected tissues.
The causative agent is Mycobacterium leprae, a rod-shaped, aerobic (oxygen-dependent) bacillus, remarkable in being unable to live freely, being only able to exist intracellularly. The bacillus was discovered in 1873, by Dr. Gerhard Hansen of Norway (Figure 7). In recognition of this fact, leprosy was also called Hansen’s disease [4]. Microscopically, M. leprae is an extremely difficult organism to stain on account of the waxy coat that prevents many stains from reaching the body of the bacterium proper. That difficulty was overcome with the introduction in 1882 of the Ziehl-Neelsen carbol-fuchsin stain that makes M. leprae appear as a red, acid-fast organism (Figure 8 A). It would be out of place to describe the staining method in detail here as such a description can be easily found in texts [3] and particularly on the web [5], instead I will discuss the microscopic findings made in the corresponding slide.

Figure 6. An old (ca 1900) picture of a leprosy patient exhibiting profuse skin lesions.
Figure 7. A late 1800s photograph of Dr. Gerhard Henrik Hansen, the discoverer of the leprosy agent.
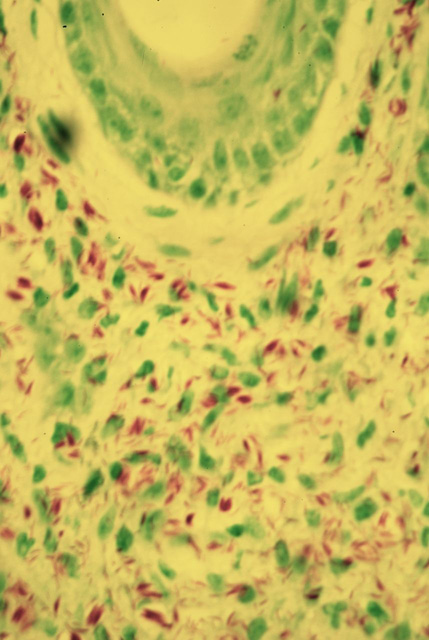
Figure 8 A. A multi-bacillary skin lesion as seen in the leprosy slide. It shows myriads of Mycobacteria, single or in clusters, stained in red by the Ziehl-Neelsen method. The V-shaped structure in the top is part of a tangential section of a hair shaft. The field eight is 170 µm.
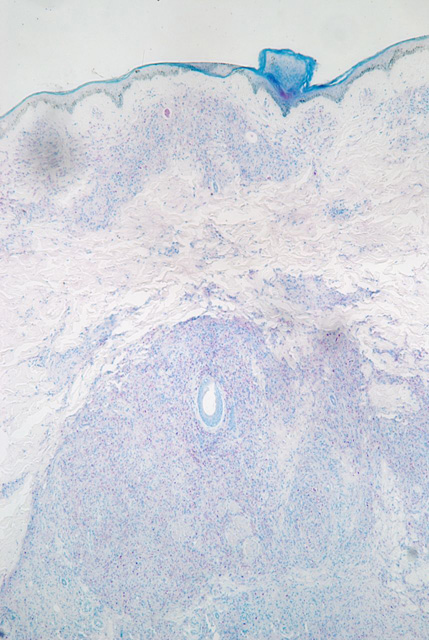
Figure 8 B. Panoramic view of the same lesion. The area seen in figure 8 A, including the section of the hair shaft is located near the center of the field. The Mycobacteria are concentrated in the dermal region (dermis) of the skin (see figure 10 for orientation). Contrast in this picture is low since the stain purposely keeps the tissue lightly stained in order to emphasize the heavily stained bacilli. The field eight is 2,100 µm.
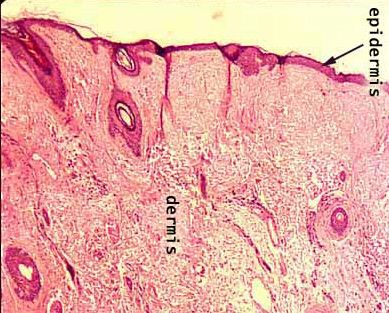
Figure 9. A view of the normal skin. A few sections of hair shafts are present, compare with the field seen in figure 8B.
This concludes the overview of the slide set and of two of the diseases represented in it. In the second part of this survey I will continue with the “apocalyptic” view of the remaining slides. I will discuss, briefly but from a general perspective, the microscopic correlation of tuberculosis, syphilis, and of a complication of the AIDS infection. This two-part series will end on a note of hope, as the book of Apocalypse does.
Comments to the author are welcomed.
APPENDIX
All the photomicrographs were taken using a Nikon D80 camera, set in manual mode and attached to an Olympus BHS microscope. Plan-apochromat objectives ranging from 4x to 40x were used. In figure 8 A, a yellow-green filter was used to enhance the red-stained bacilli. Koehler illumination was used for all pictures. Field size was measured with a 2 mm long stage micrometer. The images were digitally enhanced using Apple’s iPhoto program.
REFERENCES
1. The Book of Revelation, or Apocalypse of John. The Jerusalem Bible (1966). New Testament, pages 430-451. Doubleday & Company, Inc., Garden City, New York.
2. A Brief History of Anthrax. The Office of the Public Health Service Historian. lhncbc.nlm.nih.gov/apdb/phsHistory/resources/anthrax/anthrax.html
3. Luna, Lee G. (1992) Histopathological Methods and Color Atlas of Special Stains and Tissue Artifacts. American Histolabs, Inc., Gaithersburg, Maryland, p. 183.
4. History of Leprosy (2008). http://www.stanford.edu/group/parasites/ParaSites2005/Leprosy/history.htm
5. Ziehl-Neelsen Stain (2008). www.123exp-biology.com/t/01174369005/
Published in the September 2008 edition of Micscape.
Please report any Web problems or offer general comments to theMicscape Editor .
Micscape is the on-line monthly magazine of the Microscopy UK web site atMicroscopy-UK
© Onview.net Ltd, Microscopy-UK, and all contributors 1995 onwards. All rights reserved.
Main site is at www.microscopy-uk.org.uk
with full mirror at www.microscopy-uk.net
.