THE HORSEMEN OF THE APOCALYPSE,
A MICROSCOPIC VIEW. PART II
MANUEL
del CERRO,
Rochester, New York
MARILU
DeCOSTE,
Princeton, New Jersey
INTRODUCTION
In the first part of this article, published in the September issue of Micscape, we proposed a parallel between the agents of some deadly infectious diseases and the Horsemen of the Apocalypse, mentioned in the Book of Revelation, that brought destruction upon the Earth [1]. The idea originated from reviewing a set of slides recently purchased on eBay showing tissues infected with some very deadly diseases. The slides are signed with the initials A. J. D. These initials correspond to the name of Anthony J. DiDonato from Philadelphia.
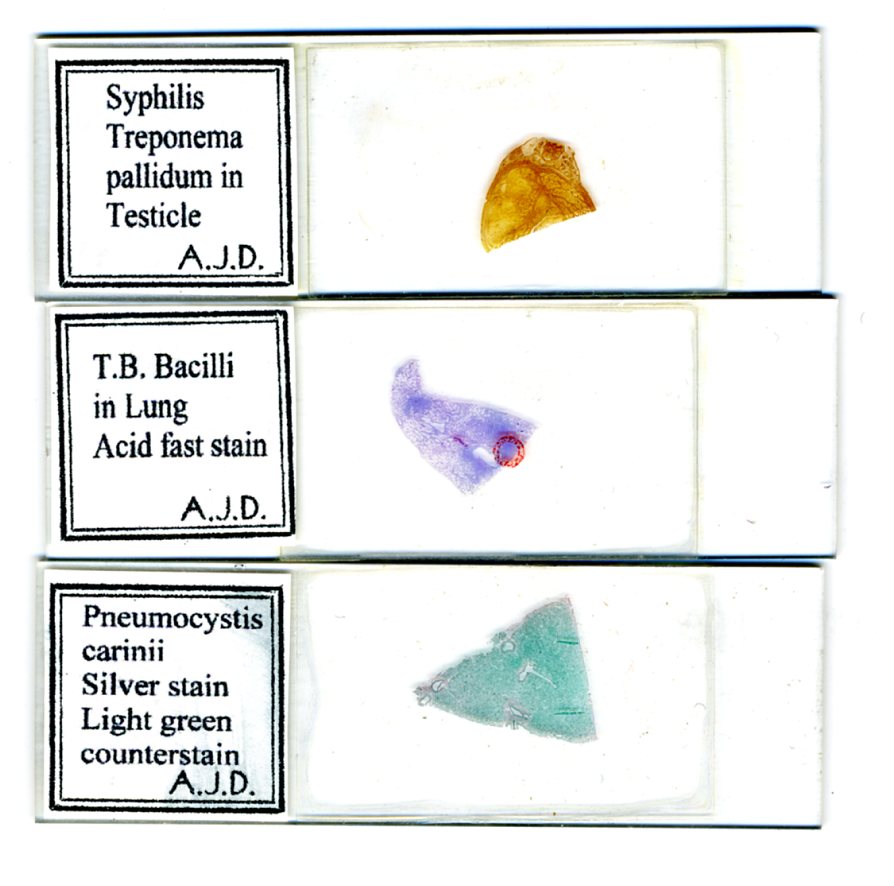
Figure 1. Scan of the three slides reviewed in this article
THE SLIDES AND THE DISEASES
In the first article I reviewed the slides of anthrax and leprosy. In this second part we will discuss those of syphilis, tuberculosis, and the P. carinii infection, as well as the historical perspective of the corresponding diseases.
SLIDE 3. SYPHILIS TREPONEMA IN TESTICLE
Until late in the 20th century, syphilis was the most dreaded of the sexually transmitted diseases. We have published an article in Micscape discussing the history of the disease [2] and the discovery of its causative agent, Treponema pallidum (Figure 2). Since that article is, almost literally just one click away, we do not need to return to those points here. Instead, we will review briefly the forms of the disease and then discuss the microscopic findings in this slide.

Figure 2. A severe epidemics of syphilis hit Europe during the early Renaissance. It was, in the medical opinion of the times, a “new disease.”
The first stage of the disease is known as primary syphilis. It is characterized by a single lesion in the skin or mucosa, at the point of penetration of Treponema. This lesion appears about three weeks after contact and it cures on its own in three to twelve more weeks. Unfortunately, this local healing does not mark the end of the disease. On the contrary, it covers the fact that the bacterium is being dispersed through the body and is multiplying actively.
If untreated, primary syphilis progresses to the next stage, secondary syphilis. This is the most contagious stage of the disease. It begins with light fever, malaise, and particularly with skin lesions (Figure 3). However, all organs of the body can eventually be affected [3].

Figure 3. We may ignore this man’s coats of arms, his flamboyant hat, or his unusual shoes, but we can not ignore his skin lesions, typical of secondary syphilis. Early 1500s drawing attributed to Albert Dürer.
The localization of the lesions and the evolution of the disease vary greatly “because the long and tenuous balance between the host and the invading spirochete” [3]. If still untreated, or treated ineffectively, the disease progresses to the stage of tertiary syphilis, which affects the cardiovascular and nervous system with devastating effects. Liver, bones, and testes can also be affected; the latter localization is relevant to the slide that we are to examine.
It was appropriate as we start searching for T. pallidum in this slide to remember that the agent can be 6 to 50 µm long but it is only 0.15 µm thick. Now 0.15 µm is at the limit of resolution of a good 100x oil immersion objective operating under ideal conditions. “Inflating” the image of the bacterium is the practical way of observing it. One such technique is dark-field that renders the bacterium self-luminous and therefore detectable (Figure 4). Dark-field microscopy permitted the discovery of T. pallidum. The technique is successful when the living Treponema is seen alive, in isolation within an exudate collected from the lesion. In a tissue section the surrounding elements interfere, therefore it is necessary to resort to different means. Impregnation with silver salts [4], as done in this slide, actually coats the bacillus with a silver precipitate, thus bringing it well within the resolving power of the light microscope.
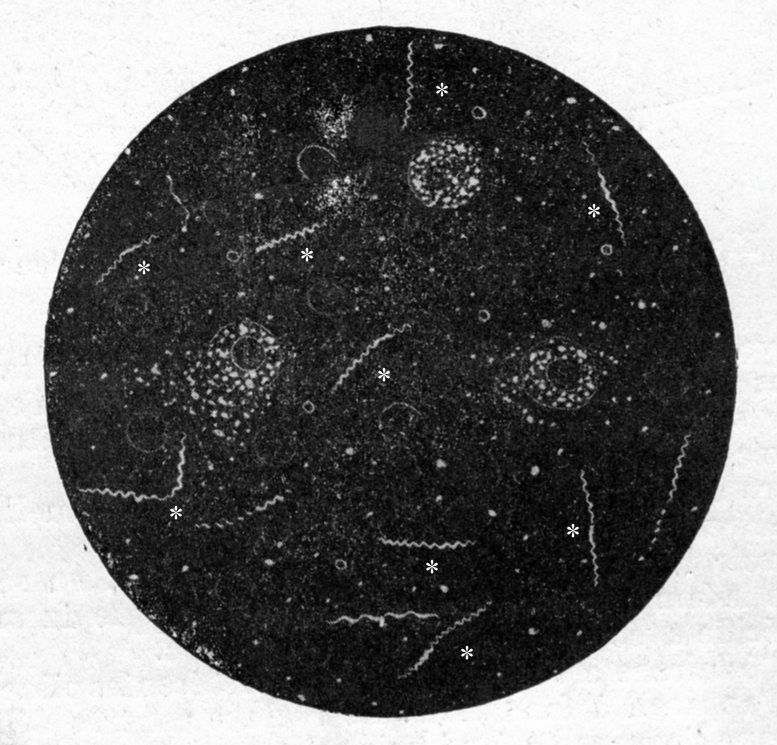
Figure 4. Digitized image of a 1910 dark-field photomicrograph. The living spirochete (indicated by asterisks) are seen clearly as bright, helical objects against the dark background; the other, round and granulated structures are cells from the host.
We searched this slide using the 40x objective. The distribution of spirochete is uneven in this section; some areas show none, but there are spots teeming with them. It is a tribute to the quality of the preparation that the Treponema can be seen with a 40x objective operating in bright field. Naturally, a better view is obtained using an oil immersion 60x NA 1.30 objective with oiled condenser (Figure 5).
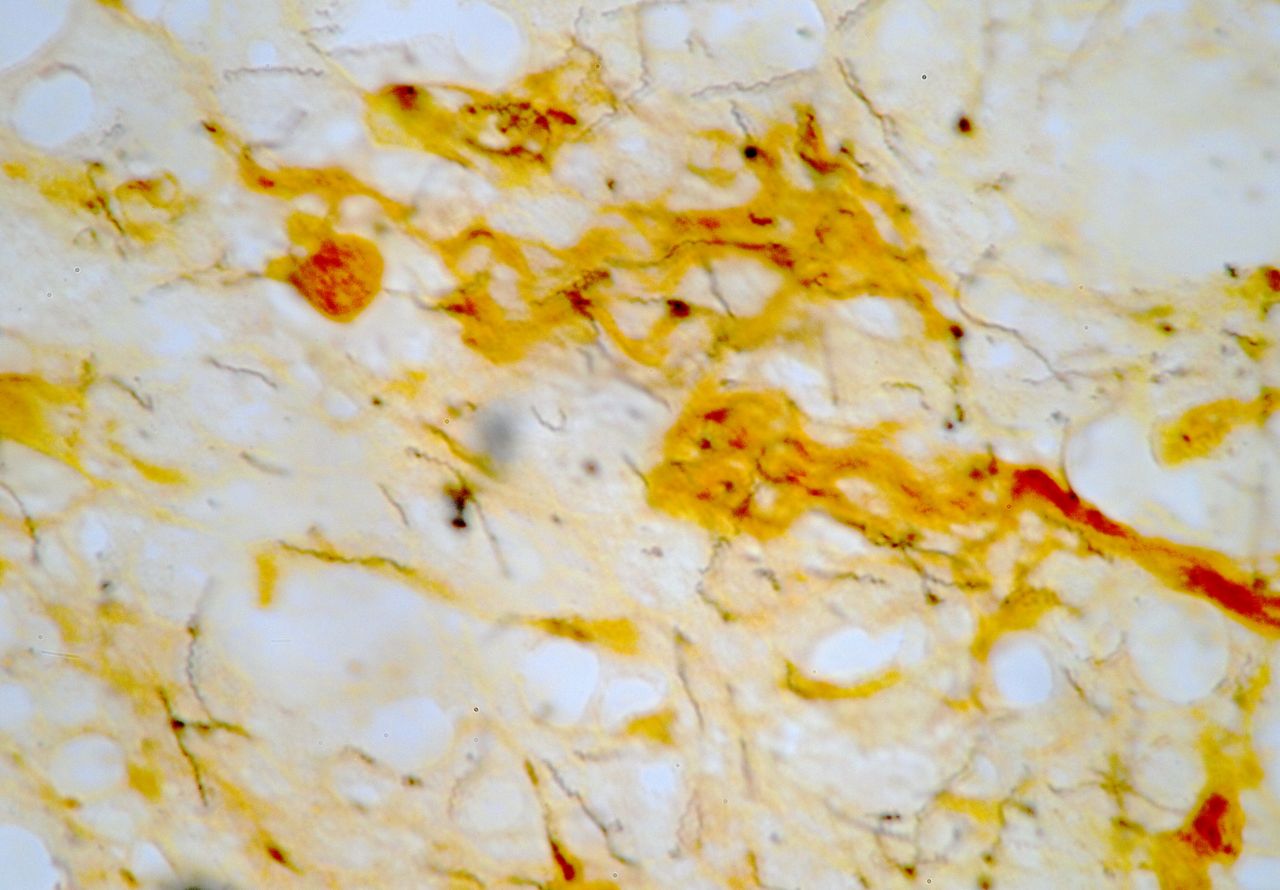
Figure 5. Treponema as seen in the Syphilis slide. Numerous treponema are present in the field; they are rendered black by the silver impregnation. The host tissue is counterstained with an unidentified gold-red stain. The section is relatively thick and thus, some of the treponema are beyond the depth of focus of the 1.30 NA objective.
SLIDE 4. TUBERCULOSIS BACILLI IN LUNG
The history of tuberculosis began twenty five centuries ago. Hippocrates recognized it around 460 BC, and named it “phthisis”, Greek for consumption. He recognized its possible fatal outcome. Knowledge advanced no further until in 1679, the medical great Sylvius described in autopsy materials, the pulmonary and extra-pulmonary lesions that are typical of the disease [5]. The next epoch-making step was due to microscopic observations. In 1882, Robert Koch applied new staining techniques and used Zeiss microscopes that were the best at best [6]. Thus, he was able to discover the agent of tuberculosis, Mycobacterium tuberculosis [7]. The role of the microscope as an instrument of discovery was crucial. In August 1884 the magazine Scientific American recognized it: “The brilliant discoveries of Pasteur and Koch are as much due to the perfected microscope as to any one cause. The nature and habits of tubercular bacillus have only been capable of study since the microscope was so improved that organisms heretofore unrecognizable stand revealed.”
Koch followed his all-important finding of the responsible microbe with rigorous experiments that proved beyond any doubt, that the Mycobacterium, and only it, could cause tuberculosis. This was one of the great moments not only in the history of medicine but in the history of the world. Why? Because in the middle-late 1800s, tuberculosis had become the scourge of industrialized Europe. Not only medical literature but art in general alluded to its horrors. Let’s remember that in Verdi’s La Traviata, Violetta dies of tuberculosis, and so does Mimi in Puccini’s La Bohème [8]. We also need to mention the exceptionally insightful view of the psychology of tuberculosis patients provided in Thomas Mann’s The Magic Mountain [9]. We must now return to the microscope, as the microscopic discovery of the causative agent is what led to the cure.
Figures 6, 7, and 8. Tuberculosis: The Clinician. The Microscopist. The Microbe.

Figure 6. The great French clinician Rene Laennec (1781-1827), introduced the stethoscope into medical practice. He is shown listening to the chest sounds of a tuberculosis patient at the Hospital Necker in Paris. Laennec contracted tuberculosis and died from the disease.

Figure 7. Robert Koch (1843-1910), the great German bacteriologist who discovered the microbe of tuberculosis in 1882.
Slide 4 shows a very abnormal lung. The air space is severely reduced and the tissue is heavily infiltrated by inflammatory cells. The red circle on the cover slip (see figure 1) corresponds to an area of advanced tissue damage; this is the area shown in figure 8.
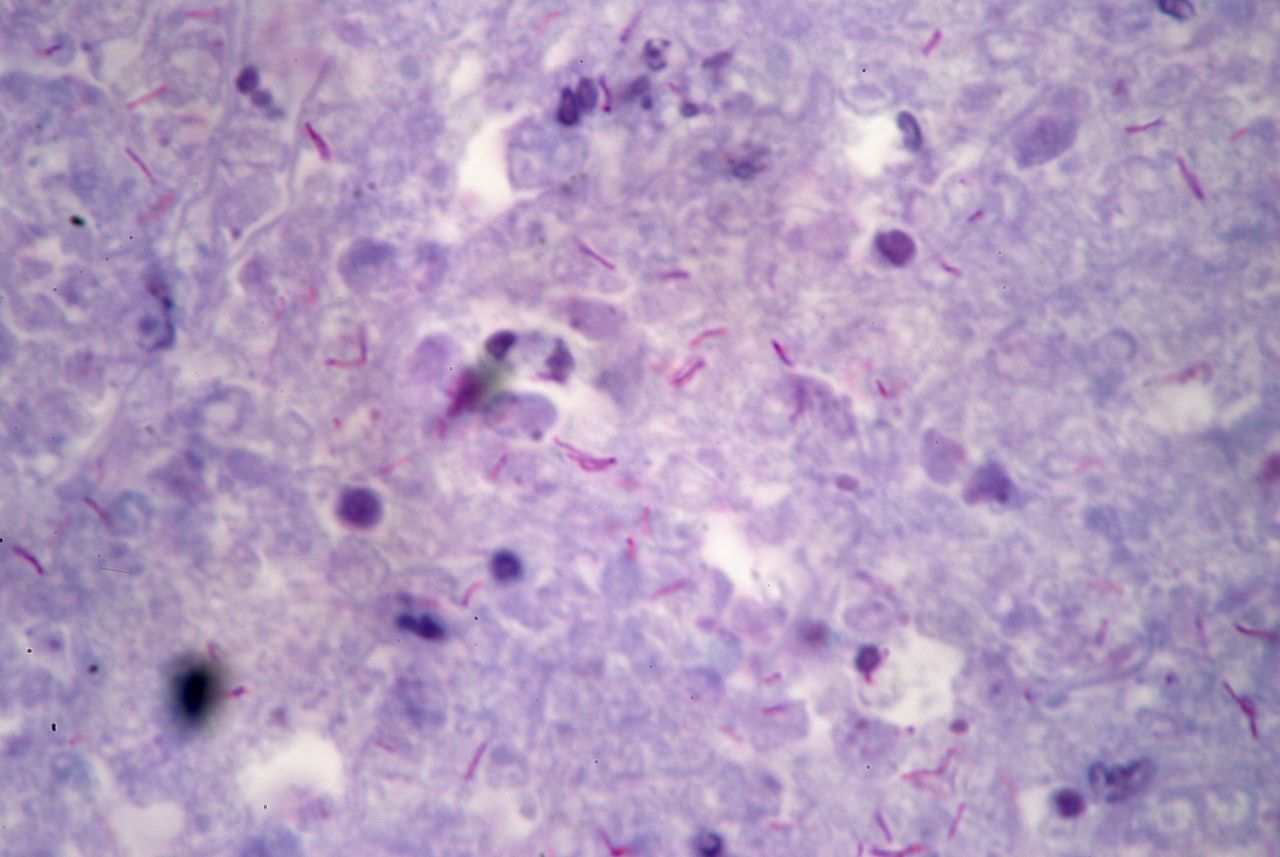
Figure 8. Photomicrograph of an advanced tuberculosis lesion in a lung. The Mycobacteria are seen as thin rods heavily stained in a shade of red. The background is formed by a few living cells stained in deep blue and by a mass of debris resulting from the extensive disintegration of host cells. No air sacs remain in this area. Field width is 170 µm.
SLIDE 5. P. CARINII IN LUNG.
The story of the Acquired Immune Deficiency Syndrome (AIDS) caused by the HIV virus is too recent and its manifestations too well known to need repetition here. However, in discussing this last slide, it is appropriate to remember that before the current multi-drug antivirus treatment, AIDS patients were often attacked by opportunistic germs. These are infectious agents that rarely, if ever, attack a healthy individual. The last slide in this set shows pneumonia caused by one of most common of these opportunistic agents, Pneumocystis carinii [10]. P. carinii is a yeast-like fungus which attacks the lungs of immunocompromised hosts, whether it be induced by the immune compromise produced by AIDS, or by chemotherapy, or drug induced in solid-transplant patients. It is a salient feature of P. carinii to produce cysts; hence the genus name, Pneumocystis. Those cysts can be easily observed in stained tissue sections; that is the case in this slide (figure 9). Impregnation of the section with silver salts results in heavy stain of the cysts. The histo-technician wisely counter-stained the section with light-green, thus outlining the tissue background without interfering with the observation of the parasite. Fortunately, the incidence of P. carinii pneumonia is declining. The current multi-drug antiviral treatment keeps AIDS patients free from P. carinii infections. Aggressive treatment effectively treats it in patients who are affected by other conditions.
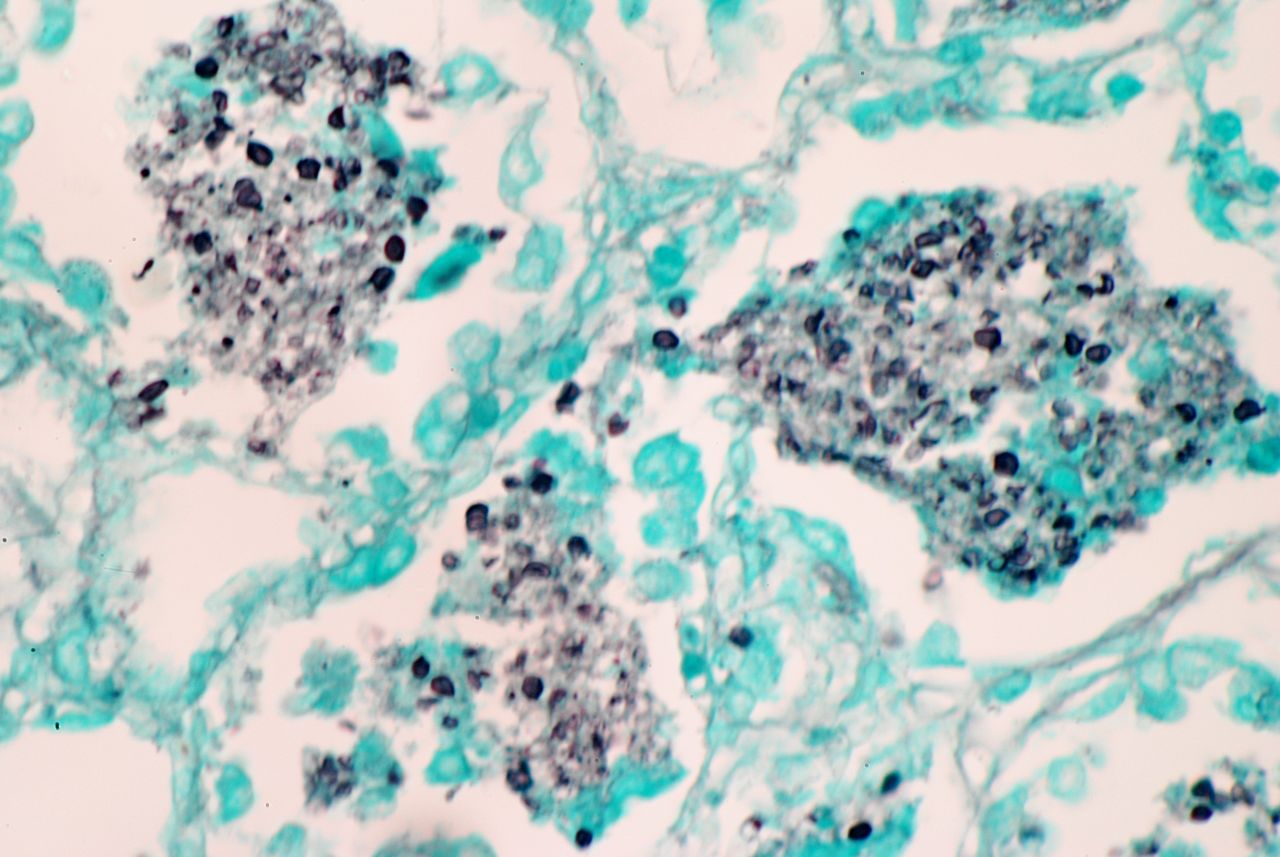
Figure 9. Three alveoili show their lumina occupied by a mass of black-stained P. carinii cysts and green stained host cells. This, and the concurrent inflamation, impair the gas-exchanging ability of the lung and induce respiratory distress. The width of the field is 420 µm.
CONCLUSION
This concludes our “apocalyptic” overview of this set of slides which includes some of the most deadly infectious agents attacking humankind. The Book of the Apocalypse duels in sorrow and death but it ends with the joyful view of a world of everlasting peace. We too will end with a note of hope. A century ago the microbes we have seen in these slides were heralds of sorrow and death. It took less than a century for microscopists and clinicians to find cures for anthrax, leprosy, syphilis, and tuberculosis. AIDS is not cured yet, but it is already under control. There is reason to hope that the present century will bring the cure, among other diseases, of Parkinson’s, cancer, macular degeneration, and Alzheimer’s. It is heart warming to think that the amateur microscopists of the 2090s will be able to see tissues affected by these conditions only by buying old slides; those made in our times. Research sustains the audacity of hope!
APPENDIX
All the photomicrographs were taken using a Nikon D80 camera, set in manual mode and attached to an Olympus BHS microscope. Plan-apochromat objectives ranging from 4x to 60x were used. Köhler illumination was used for all pictures. Field size was measured with a 2 mm long stage micrometer. The images were digitally enhanced using Apple’s iPhoto program.
Comments to the author are welcomed.
REFERENCES
1. The Book of Revelation, or Apocalypse of John. The Jerusalem Bible (1966). New Testament, pages 430-451. Doubleday & Company, Inc., Garden City, New York.
2. del Cerro, Manuel and Lazaros C. Triarhou (2007) Syphilis and the Microscope, a Century-Long Relationship. Micscape, December issue.
3. Sparling, P. Frederick (1991) Syphilis. Ch. 340, pp. 1761-1770 in: Cecil Textbook of Medicine, 19th Edition, W. B. Saunders Co., Philadelphia.
4. Luna, Lee G. (1992) Histopathological Methods and Color Atlas of Special Stains and Tissue Artifacts. American Histolabs, Inc., Gaithersburg, Maryland, p. 223 (syphilis) and pp. 183-184 (tuberculosis).
5. NJMS Tuberculosis Center. Brief History of Tuberculosis (1996).
6. Münch, Raghild and Georg Kroiss (1998) One of Robert Koch’s Microscopes in Africa. Innovation 5: 19-21.
7. Lechevalier, Hubert A. and Morris Solotorovsky (1974) Three Centuries of Microbiology. Ch 3, Koch. Dover Publications, Inc., New York, pp. 536.
8. Newman, Ernest (1930) Stories of the Great Operas and Their Composers. pp 641 & 842.
9. Mann, Thomas (Woods’ translation, 1996) The Magic Mountain. Knopf Publishing Group, pp. 720.
10. Wilkin, Aimee and Judith Feinberg (1999) Pneumocystis carinii Pneumonia: A Clinical Review. Amer. Family Physician, 60: 1699-1708.
Published in the October 2008 edition of Micscape.
Please report any Web problems or offer general comments to theMicscape Editor .
Micscape is the on-line monthly magazine of the Microscopy UK web site atMicroscopy-UK
© Onview.net Ltd, Microscopy-UK, and all contributors 1995 onwards. All rights reserved.
Main site is at www.microscopy-uk.org.uk
with full mirror at www.microscopy-uk.net
.